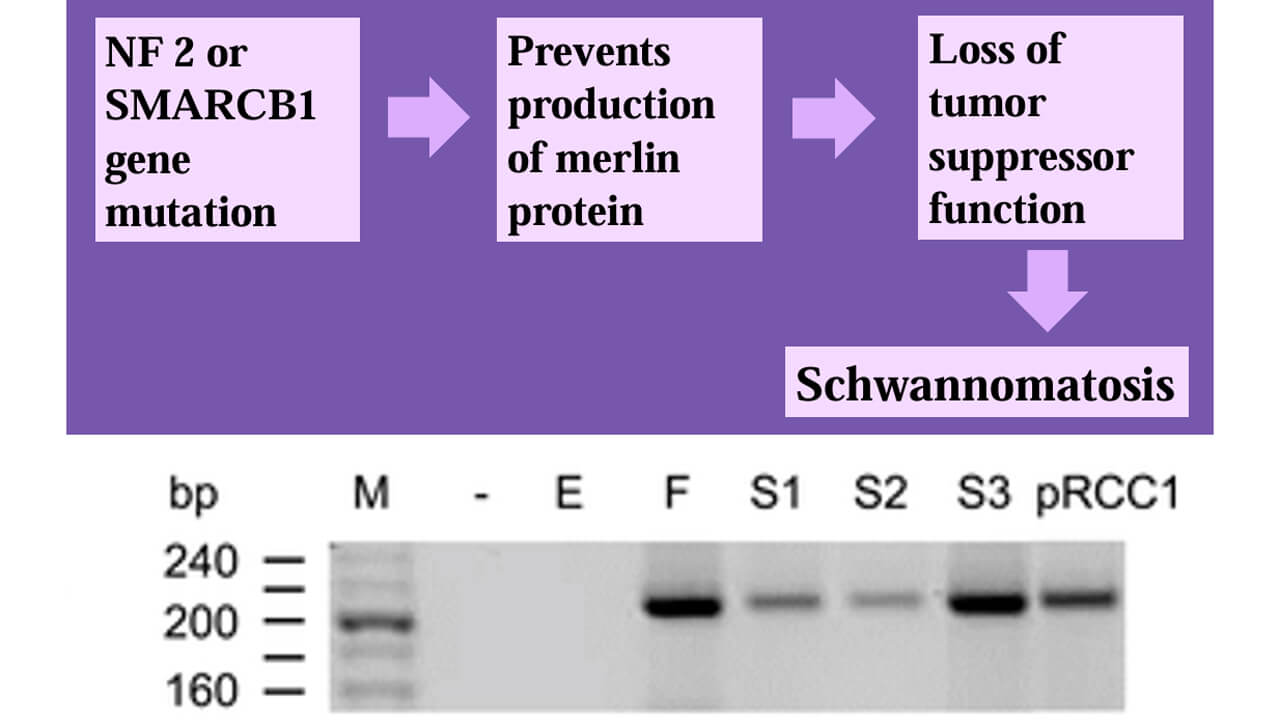
Figure 1. Genetics of RCC and Schwannoma^8
Physician Assistant (PA)
Physician Assistant (PA)
This project was completed for PY 652: Medical Writing & Biostatistics for PA.
This work by Madeline Folsom '23, MHS ‘25 covers treatment and diagnostic challenges with pelvic schwannoma as well as the significance of the proposed genetic connection between pelvic schwannoma and renal cell carcinoma.
Physician Assistant
School of Health Sciences
History:
Physical Exam:
Vitals:
Pre-operative:
Post-operative:
Pre-Operative Differential Dx:
Labs/Diagnostics:
Procedures:
Figure 1. Genetics of RCC and Schwannoma^8
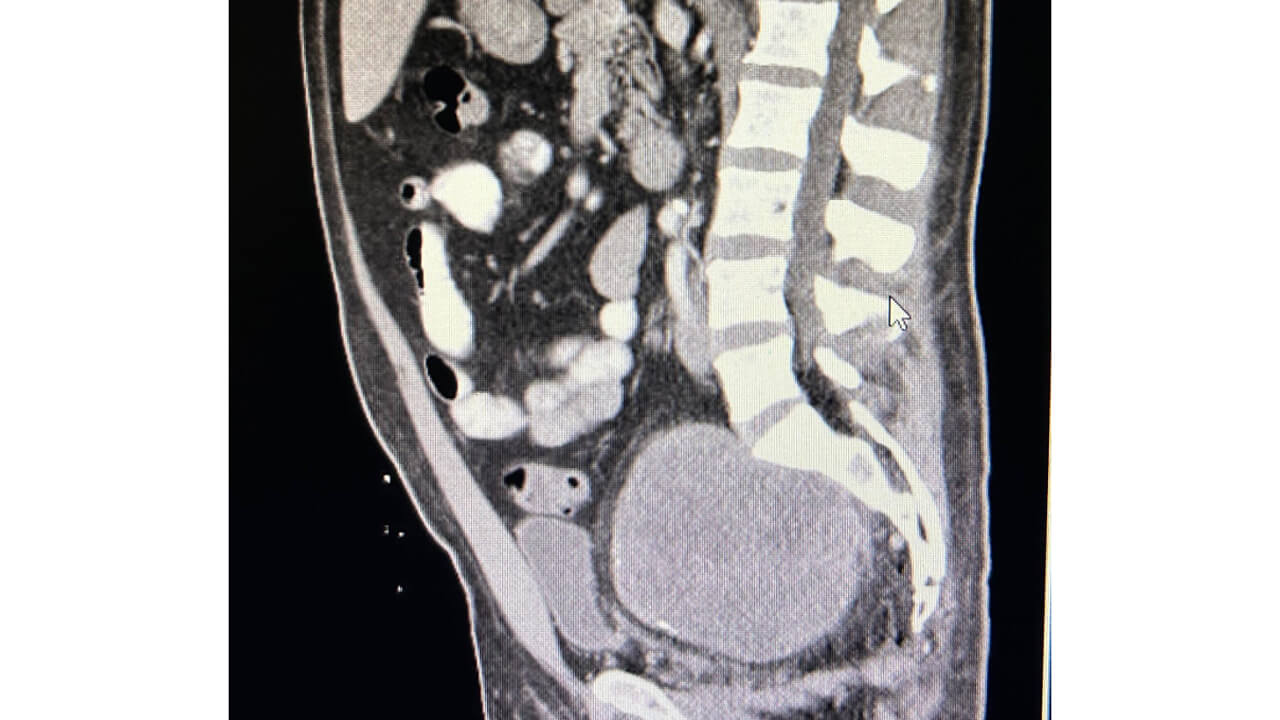
Figure 3. Pre-op sagittal CT
"My biggest takeaways from this experience included gaining an in depth understanding of the process of diagnosing and treating this rare tumor, learning the value of each member’s role on the interdisciplinary healthcare team, and the importance of creating presentations like this one to share with the medical community to contribute to the lifelong learning of all healthcare providers. I found that this whole process from seeing the patient for the first time, to assisting with his surgery, to creating this presentation all held valuable lessons and provided me with growth in all of the skillsets that will help me become best provider I can be in my future career as a PA." - Madeline Folsom '23, MHS '25
This serves as an overview of the project and does not include the complete work. To further discuss this project, please email Madeline Folsom.
PY 652: Medical Writing & Biostatistics for PA introduces biostatistics, evidence-based medicine, as well as critical review and application of evidence to clinical decision-making. Students learn to construct clinical questions and perform literature searches. Methods for critically appraising the literature and strategies for maintaining currency of medical knowledge through journal clubs are practiced. Review of basic techniques of medical writing and presentation allow students to develop presentations, posters and journal articles while incorporating peer review feedback.
We've sorted each of our undergraduate, graduate and doctoral programs into unique Areas of Interest. Explore these categories to discover which programs and delivery methods best align with your educational and career goals.
Explore Health and Medicine at Quinnipiac
References
1. Deng C, Wang P, Liu Y, et al. Laparoscopic resection of pelvic schwannomas: a 9-year experience at a single center. World Neurosurgery: X. 2022;17:100150. doi:10.1016/j.wnsx.2022.100150
2. Yin M, Wang W, Rosenberg J, et al. Targeted therapy in collecting duct carcinoma of the kidney: A case report and literature review. Clinical Genitourinary Cancer. 2016;14(2). doi:10.1016/j.clgc.2015.11.008
3. Pan S, Wang P, Chen Z, Liu Y, Zhou Z. Retroperitoneal schwannoma mimicking a metastatic lymph node of renal clear cell carcinoma: a case report. Front Neurol. 2024;15:1450217. Published 2024 Aug 2. doi:10.3389/fneur.2024.1450217
4. Colecchia L, Lauro A, Vaccari S, et al. Giant pelvic schwannoma: case report and review of the literature. Dig. Dis. and Sci. 2020;65(5):1315-1320. doi:10.1007/s10620-020-06128-2
5. Kawahori T, Mukai S, Saito Y, Nishida T, Fukuda T, Ohdan H. A rare case of giant pelvic retroperitoneal schwannoma. Radiol. Case Rep. 2024;19(12):5738-5743. doi:10.1016/j.radcr.2024.08.109
6. Kalagi D, Bakir M, Alfarra M, Aborayya A, Anwar I. Two unusual presentations of presacral schwannoma; a case series. Int. J. Surg. Case Rep. 2019;61:165-168. doi:10.1016/j.ijscr.2019.07.042
7. Handa K, Ozawa H, Aizawa T, et al. Surgical management of giant sacral schwannoma: a case series and literature review. World Neurosurg. 2019;129. doi:10.1016/j.wneu.2019.05.113
8. Hulsebos TJM, Kenter S, Baas F, et al. Type 1 papillary renal cell carcinoma in a patient with schwannomatosis: mosaic versus loss of SMARCB1 expression in respectively schwannoma and renal tumor cells. Genes, Chromosomes, and Cancer. 2016;55(4):350-354. doi:10.1002/gcc.22338
9. Klose C, Gibbs M, Kahn A, Baird B, Farres S, Zganjar A. Diagnosis and open excision of concurrent pelvic schwannoma and chromophobe renal cell carcinoma. Urol. Case Rep. 2024;56:102809. doi:10.1016/j.eucr.2024.102809